CASE REPORT | https://doi.org/10.5005/jp-journals-10077-3020 |
From Disharmony to Harmony: Management of Impacted Central Incisor with the Combined Surgical and Orthodontic Approach
1–4Department of Pedodontics and Preventive Dentistry, Saraswati Dental College and Hospital, Lucknow, Uttar Pradesh, India
Corresponding Author: Shagun Agarwal, Department of Pedodontics and Preventive Dentistry, Saraswati Dental College and Hospital, Lucknow, Uttar Pradesh, India, Phone: +91-8707753716, e-mail: shagungrwl@gmail.com
How to cite this article Agarwal S, Pandey SN, et al. From Disharmony to Harmony: Management of Impacted Central Incisor with the Combined Surgical and Orthodontic Approach. J South Asian Assoc Pediatr Dent 2019;2(1):1–4.
Source of support: Nil
Conflict of interest: None
ABSTRACT
Introduction: Supernumerary teeth in the maxillary midline are common. Early detection of such teeth is important if pathological complications are to be avoided. Supernumerary teeth are the main cause of impaction of maxillary incisors. Impacted maxillary incisors can have a major impact leading to dentofacial malocclusion in an individual.
Case report: In this reported case, the occlusal radiographic view of a 10-year-old boy revealed an impacted supernumerary tooth in the maxillary anterior region, which was interfering with the eruption of the permanent left central incisor. The impacted supernumerary tooth was surgically removed, and the impacted maxillary left central incisor was moved into its proper position with surgical exposure and orthodontic traction force, after which it showed excellent stability.
Conclusion: Impaction of the maxillary permanent incisor is not a frequent case in pediatric dentistry, but its treatment is challenging because of the importance of these teeth in facial esthetics and developing child psychology.
Keywords: Impacted incisor, Orthodontic traction, Surgical exposure, Supernumerary tooth.
INTRODUCTION
A smile of a child is a packaged sunshine and rainbows. The missing maxillary central incisor is a significant matter of esthetic and practical concern for an individual. The frequency of maxillary central incisor impaction has been found to be within a range of 0.006–0.2% in the age group of 5–12 years.1
Tooth impaction may result from several local causes. Causes of impactions are the following:2
- Arch length discrepancy
- Presence of supernumerary teeth
- Mucosal or bony barrier
- Retained deciduous teeth.
Supernumerary teeth are the leading cause of impaction of the maxillary central incisor. The supernumerary teeth (hyperdontia) is a state which can be defined as any teeth-like substance in excess of the typical configuration of the standard number of deciduous or permanent teeth.3,4 When impaction occurs, surgical removal of the supernumerary tooth is always indicated. After the removal of the supernumerary tooth from the path of eruption, an impacted tooth either erupts spontaneously if it has conserved its eruptive force or orthodontic force is required to bring the tooth in normal position.5
CASE DESCRIPTION
A 10-year-old boy reported with the chief complaint of missing upper left front tooth since the past 4–5 years. The child was physically healthy and had no history of any medical and dental trauma or extraction.
On clinical examination, a missing maxillary permanent left central incisor (Fig. 1) was seen with no apparent arch length discrepancy in both maxillary and mandibular arches. The patient had a skeletal class I malocclusion and a balanced facial pattern. Intraoral examination revealed a mixed dentition phase with an Angle’s class I molar relationship.
Maxillary radiographic occlusal view further revealed a supernumerary tooth with an impacted permanent central incisor on the left side of the maxillary arch (Fig. 2).
The treatment plan was explained to the patient and his parents. They agreed for the extraction of supernumerary tooth surgically followed by surgical exposure of impacted central incisor and alignment of the left impacted incisor into the arch with orthodontic treatment. Informed consent was obtained for the same from the parents.
Before the beginning of the surgical phase, full mouth oral prophylaxis was done, and the patient was advised to go for a regular medical check-up, his complete blood picture routine investigation was done. Surgery was planned for the next day. Under local anesthesia, crevicular and vertical incisions were given using surgical blade number #15, and #11 and a full-thickness mucoperiosteal flap on the labial side was raised using a periosteal elevator (Figs 3 and 4).

Fig. 1: Clinical image showing the unerupted maxillary left central incisor

Fig. 2: Occlusal radiograph showing the supernumerary tooth with the impacted tooth 21

Figs 3A and B: Operative view showing impacted central incisor with supernumerary teeth on raising the labial mucoperiosteal flap

Fig. 4: Extracted supernumerary tooth
The supernumerary tooth and impacted central incisor tooth were identified followed by the removal of supernumerary tooth surgically using extraction forceps; further, the extraction socket was gently curetted for any pathological remnants of dental sac followed by bonding of lingual button on the labial side of the impacted central incisor tooth 21. Orthodontic bands were placed on the maxillary first permanent molars on both the sides of jaw along with the placement of Begg brackets on all maxillary anterior and posterior teeth followed by the placement of the 0.014 NiTi round archwire leaving a tied ligature wire from the impacted tooth 21 which was bended in the form of a hook around the archwire to avoid trauma to oral tissues (Figs 5 to 7). This was followed by approximation of the reflected mucoperiosteal flap with (3-0) black silk sutures for a week. Instructions were given not to disturb the surgical site till healing. After 1 week, sutures were removed and light continuous orthodontic traction force (60–90 g) was applied by twisting the ligature wire in the subsequent visits to align the impacted central incisor in the occlusal plane.
The patient was recalled after 1 month, and intraoral periapical radiograph was taken, showing the movement of impacted tooth mesially and incisally (Fig. 8).
After 3 months, again a radiographic investigation was done, which showed the satisfactory movement of impacted tooth 21 toward the occlusal plane (Fig. 9).
Every month the patient was recalled for the activation of the ligature archwire to apply continuous orthodontic extrusion force on the impacted tooth 21. After 10 months of follow-up, the impacted tooth 21 has completely erupted in the oral cavity and the lingual button was then replaced with the Begg bracket on tooth 21, and the 0.014 NiTi archwire was replaced with the 0.016 NiTi round archwire for leveling and finishing (Fig. 10).
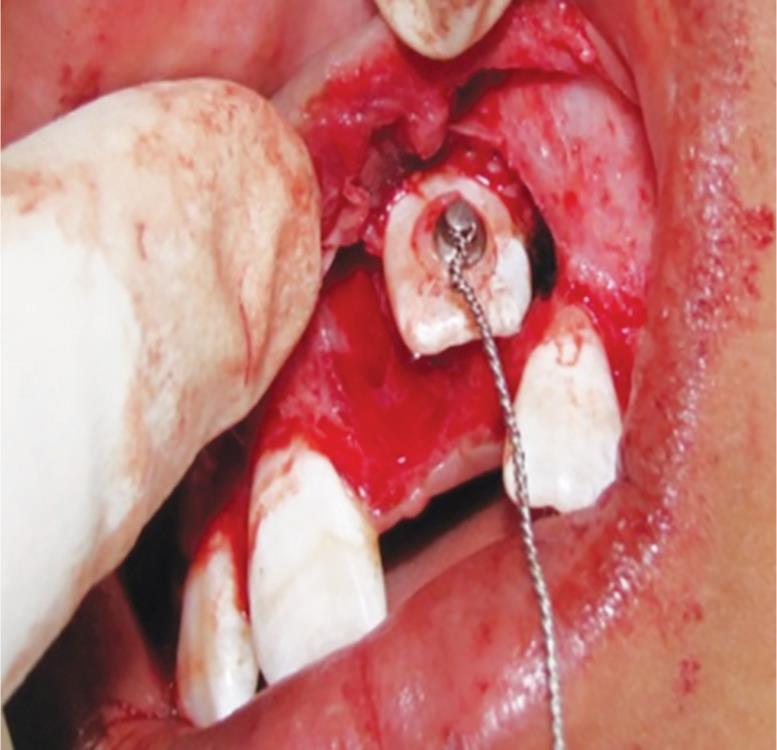
Fig. 5: Lingual button was bonded on the impacted tooth 21 with suspended ligature wire followed by the placement of the 0.014 NiTi round archwire leaving a tied ligature wire with a hook protruding through the mucosa

Fig. 6: Lingual button was bonded on the impacted tooth 21 with suspended ligature wire followed by the placement of the 0.014 NiTi round archwire leaving a tied ligature wire with a hook protruding through the mucosa

Fig. 7: After a week, the patient was recalled, and sutures were removed followed by light continuous force application through activation of the ligature wire to the archwire
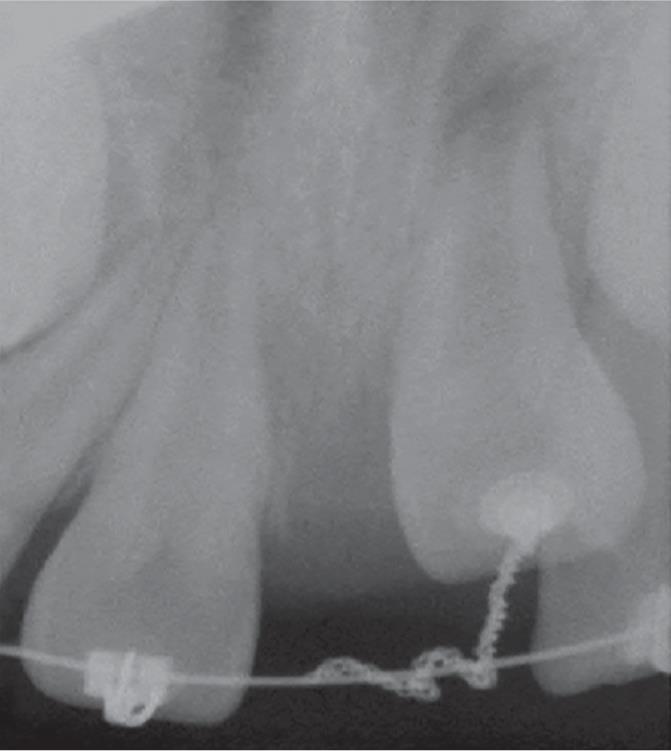
Fig. 8: Intraoral periapical radiograph showing movements of tooth 21 after 1 month and 3 months toward the occlusal plane

Fig. 9: Intraoral periapical radiograph showing movements of tooth 21 after 1 month and 3 months toward the occlusal plane

Fig. 10: Complete eruption of impacted tooth 21 in the oral cavity after 10 months
After 11 months of clinical and radiographic follow-up, the impacted tooth 21 has successfully erupted in the dental arch with a sufficient amount of attached gingival and acceptable gingival contour along with the vital pulp. Active treatment to close the diastema, in this case, was postponed until the complete eruption of the permanent maxillary canines because the attempt to close the midline diastema before the eruption of permanent canine can cause root resorption of the lateral incisor (Fig. 11). Hawley’s appliance with sufficient space for the eruption of canine was delivered for retention.

Fig. 11: Postoperative clinical image after debonding of brackets after 11 months showing the closure of the present case
The patient is under continued periodic monitoring after the permanent maxillary canines erupt, the condition will be reevaluated, and appropriate treatment will be taken as needed to close the midline space with final orthodontic alignment and leveling. Hence, the case is under regular follow-up.
DISCUSSION
The impaction defines a tooth that cannot or will not erupt into its normal functional position in time.5 Failure of complete eruption of maxillary incisors is one of the most common complications of the presence of supernumerary teeth in the anterior maxilla. Timely removal of mesiodens and with adequate space, spontaneous eruption of upper incisors have been found to occur in about 54–6% of the cases.6,7 However, the complete eruption of impacted maxillary incisor may take up to 3 years till the root formation is completed, and orthodontic treatment may be required to achieve proper positioning of the erupted tooth in the dental arch.8 In the present case, root formation for impacted incisor was not complete, so spontaneous eruption would be challenging to achieve; hence, combined surgical exposure with orthodontic extrusion treatment was planned.
According to Becker, three ways of surgical exposure for the impacted tooth9,10 are the following:
- Oral mucosa overlying the impacted tooth may be circularly excised
- Incorporating the attached gingival covering the impacted tooth by repositioning the raised flap apically
- Closed eruption technique: flap raised, incorporating the attached gingiva, and is replaced back in its former position entirely after bonding an attachment to the impacted tooth.
Favorable results have been achieved with the closed eruption technique as the aesthetic and periodontal outcome is far more superior when compared with the other two techniques.10 In the present case, the closed eruption technique was used as the raised flap was sutured back in its former position with an orthodontic attachment on impacted central incisor tooth for a better and esthetic gingival margin. The continuous extrusion force applied to the impacted central incisor in the present case was very light. This may have accounted for the maintenance of vitality of the impacted tooth post-alignment. The only disadvantage of combined surgical/orthodontic therapy is that it requires longer treatment time period, and some complications including ankylosis, nonvital pulps, and root resorption, which may be encountered at the end of the treatment.10
In the present case, the patient showed a standard clinical crown length with acceptable gingival contour. The aligned maxillary central incisor also responded normally to percussion and mobility and pulp vitality testing. However, final finishing and alignment to close the midline diastema in the current case are postponed until the eruption of permanent maxillary canines. Hence, the case is under regular periodic monitoring. This is again a limitation for doing combined surgical and orthodontic extrusion in mixed dentition cases as the treatment time is prolonged.
CONCLUSION
Maxillary left permanent central incisor was successfully repositioned in the arch by combined surgical exposure and orthodontic traction after which it showed good stability and retention with sufficient width of attached gingiva.
REFERENCES
1. Lin YT. Treatment of an impacted dilacerated maxillary central incisor. Am J Orthod Dentofacial Orthop 1999;115:406–409. DOI: 10.1016/S0889-5406(99)70260-X.
2. Congialosi TJ. Management of maxillary central incisor impacted by a supernumerary tooth. J Am Dent Assoc 1982;105:812–814. DOI: 10.14219/jada.archive.1982.0476.
3. Foley J. Surgical removal of supernumerary teeth and the fate of incisor eruption. Eur J Paediatr Dent 2004;5:35–40.
4. Prabhu NT, Munshi AK. Surgical management of labially placedpermanent maxillary central incisor after supernumerary tooth extraction; report of a case. J Clin Pediatr Dent 1997;21:201–203.
5. Bishara SE. Impacted maxillary canines: a review. Am J Orthod Dentofacial Orthop 1992;101:159–171. DOI: 10.1016/0889-5406(92)70008-X.
6. Tanaka E, Watanabe M, et al. Orthodontic traction of an impacted maxillary central incisor. J Clin Orthod 2001;35:375–378.
7. Vanarsdall R, Corn H. Soft tissue management of labially positioned unerupted teeth. Am J Orthod 1977;72:53–64. DOI: 10.1016/0002-9416(77)90124-5.
8. Kocadereli I, Turgut MD. Surgical and orthodontic treatment of an impacted permanent incisor: a case report. Dent Traumatol 2005;21:234–237. DOI: 10.1111/j.1600-9657.2005.00304.x.
9. Ferrazzano GF. An impacted central incisor due to supernumerary teeth: a multidisciplinary approach. European J Paediatr Dent 2014;15(2):187–190.
10. Becker A, Brin I, et al. Closed eruption surgical technique for impacted maxillary incisors: a postorthodontic periodontal evaluation. Am J Orthod Dent facial Orthop 2002;122(1):9–14. DOI: 10.1067/mod.2002.124998.
________________________
© The Author(s). 2019 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted use, distribution, and non-commercial reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.